Osteoarthritis
What is osteoarthritis?
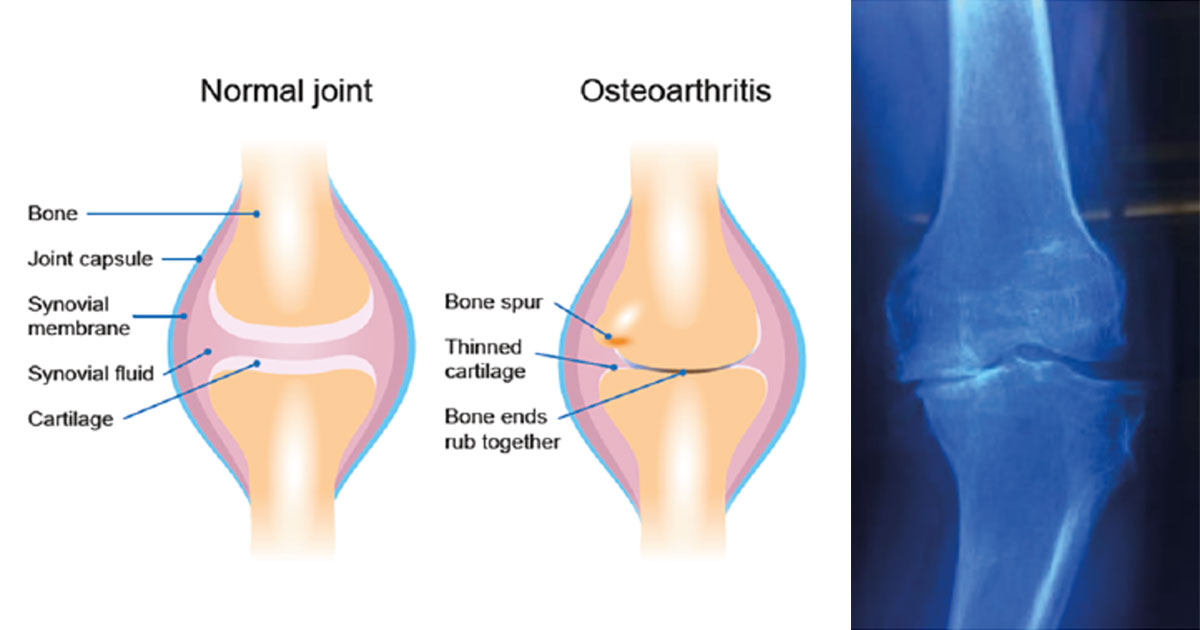
Osteoarthritis (also known as OA) is a common joint disease that most often affects middle-age to elderly people. It is commonly referred to as "wear and tear" of the joints, but we now know that OA is a disease of the entire joint, involving the cartilage, joint lining, ligaments, and bone. Although it is more common in older people, it is not really accurate to say that the joints are just “wearing out.” It is characterized by breakdown of the cartilage (the tissue that cushions the ends of the bones between joints), bony changes of the joints, deterioration of tendons and ligaments, and various degrees of inflammation of the joint lining (called the synovium).
Osteoarthritis symptoms can usually be managed, although the damage to joints can’t be reversed. Staying active, maintaining a healthy weight and some treatments might slow progression of the disease and help improve pain and joint function.
Weight loss and exercise are useful in OA. Excess weight puts stress on your knee joints and hips and low back. For every 10 pounds of weight you lose over 10 years, you can reduce the chance of developing knee OA by up to 50 percent. Exercise can improve your muscle strength, decrease joint pain and stiffness, and lower the chance of disability due to OA.
Symptoms
Symptoms commonly include:
- stiffness in the morning or after prolonged sitting
- pain with prolonged periods of walking or standing
- difficulty with activities such as stair climbing and stair descending
- joint swelling
- clicking, clunking, crunching or catching within the joint
- reduced joint flexibility (bending or straightening)
- altered joint shape and size
- altered leg posture (eg, ‘knock knees’ or ‘bow legs’)
- a feeling of instability or giving way in the knee
- feeling of weakness in the leg muscles, especially the quadriceps (front of thigh).
Knee OA symptoms commonly fluctuate, sometimes being better or worse, depending on activity. The symptoms may initially only be with activity but as OA progresses, knee pain may be experienced at rest or during the night.
Imaging techniques such as X-ray and MRI also play a role in diagnosing knee OA, though it is important to note that knee symptoms may not always match the imaging findings. Some people have quite troubling knee symptoms without much change on X-ray, whereas some people may have findings of advanced OA on their scans, though not be troubled much by pain. Treatment is dictated more by the individual person’s symptoms than their scans.
Physiotherapy and Osteoarthritis
There is good evidence to support physiotherapy management of knee OA. The main areas supported by research include:
Physiotherapy vs arthroscopy for knee OA
Physiotherapy exercise and education, combined with standard medical care (simple pain medication) is equally effective to keyhole knee surgery (arthroscopy) in the management of knee OA. In people with moderate to severe knee OA, it has been found that arthroscopy added no additional benefit in terms of physical function, pain or quality of life, when compared to physiotherapy and simple medication. In addition, physiotherapy has been shown to have minimal risk of negative side effects compared to surgery.
Your physio will provide you with information with regard to osteoarthritis, as well as provide you with an appropriate exercise programme encompassing control, stability strengthening and stretching exercises. Manual physiotherapy techniques can include soft tissue massage, dry needling and passive stretching.
Surgery
Surgical treatment becomes an option for severe cases. This includes when the joint has serious damage, or when medical treatment fails to relieve pain and you have major loss of function. Surgery may involve arthroscopy, repair of the joint done through small incisions (cuts). If the joint damage cannot be repaired, you may need a joint replacement.

A client's X-ray pre knee replacement surgery showing the “bow” knees. The client underwent a bilateral knee replacement (both knees at once) and the resulting “straightening”post operatively.
Physiotherapy pre and post-surgery
Prehabilitation
Various studies have looked at programs of strength, movement control and cardiovascular exercise for 6–8 weeks prior to total knee replacement surgery. Most studies have found improvements in post-operative pain and function in the few months following surgery, and some have shown reductions in length of hospital stay. Some of the main reasons for these outcomes include patients entering surgery with a better baseline of physical conditioning and better mental preparedness. Your physiotherapist can provide you with a specific pre operative exercise programme.
Rehabilitation
Post surgery, throughout every stage of the recovery process, physiotherapy is necessary. Working with a physiotherapist not only helps with pain relief, bit also helps you strengthen the muscles in your knee, improve your range of motion (ROM), resume independent living sooner and avoid potential complications.